Coronavirus.
A medical professional would know how the meaning of this word has
changed drastically in the past 3 months. From being the virus that
causes ‘common cold’, to today- where it has killed over 13000 people
worldwide, and it’s just getting started. The novel coronavirus
(2019-nCov or SARS-CoV2) is the latest from the family of viruses known
as ‘coronaviridae’. This family is notorious for causing respiratory disease outbreaks, second only to the Influenza family of viruses.
India.
A country of 1.34 billion (134 crore), with much of this population
living in poor hygiene and clustered environments. Developed countries
like Italy and US are struggling to meet the healthcare demands
coronavirus has produced. Needless to say, the health system of India is
grossly under-equipped to handle a blow of the same magnitude.
Mix these two. It is a recipe for disaster. Let us see how.
If
you are not a medical professional, you can ignore the jargon in
between. I will go on to explain everything in simplified terms.
India cases and fatality forecast through predictive modelling
Epidemics
grow exponentially, not linearly. Most of you would already know this.
But even then, many of us will be surprised when we see the increasing
number of daily new cases a week from now. That is, the human mind does not comprehend exponential growth very well.
To make more sense of what we should expect in the coming weeks-months,
let us take a look at a mathematical model of the same. The model used
here is the SEIR model, which has been used to accurately predict previous outbreaks like SARS.
Before
we start predicting stuff, we need to know the input parameters first-
the stats we feed into the model. The first one is R0 (R-naught) also called the Basic Reproduction Number.
It is essentially the number of new cases a single infected person will
cause during their infectious period. It is one of the most important
parameters for assessing any epidemic- it indicates how contagious the
virus is. Coronavirus has an R0~2.4. In contrast, the H1N1 virus had an
R0~1.5 in the 2009 swine flu epidemic. The R0 will inform us about how
many people will get infected.
The second one is the Case Fatality Rate (CFR),
which is the percentage of infected people that will die due to the
infection. The CFR for coronavirus has been reported between 0.5–4%. The
higher values are more appropriate in resource poor settings where the
quality of hospital and intensive care might be constrained(developing
countries), or in places where the epidemic caused a sudden surge in the
number of cases requiring critical care which overwhelmed the otherwise
sufficient healthcare system (developed countries like Italy and USA).
To achieve the lower end of CFR, early and definitive intervention to
prevent the sudden surge is needed, as seen in areas of China outside
Hubei (origin of the epidemic) and in South Korea, both of which saw a
CFR ~1%. The CFR will inform us about how many people will die.
I
must stress that estimations of an ongoing epidemic are only rough
estimations, as we still don’t know the definite parameters of this
viral disease. The point here is not to give you
pinpoint numbers, but to put in context the magnitude of the problem we
face and how different steps we take can bring a change in those
numbers.











The power of social distancing! Take a look at the effect on branches on the extreme right. (graphic by Toby Morris and Siouxsie Wiles)
The references for the parameters used has been provided at the end of the article.


Graph 1- Predicting the coronavirus outbreak in India using Epidemic Calculator (http://gabgoh.github.io/COVID/index.html) in absence of any interventions. The pink bars are the number of active infections at any given time (and not the cumulative cases upto that time) , and the blue bars are the cumulative deaths. The input parameters are mentioned below the graph, based on the latest available research (reference at end of article). Important parameters include an R0=2.4 and Case Fatality Rate=4%. I encourage you to use this calculator and play with your own values to learn more.
This is what happens if no interventions are done to control coronavirus spread, ie, the worst case scenario for India. About 115,00,00,000 (115 crore) people are infected in total,
which is about 85% of India’s population. In the process, the health
system is overwhelmed and people lose their lives en-masse: total deaths ~ 4,50,00,000 (4.5 crore).
This happens across a span of about 6 months, assuming a hypothetical
scenario where no interventions are done at all and the disease is
allowed to spread freely.

Graph 2- Predicting the coronavirus outbreak in India using Epidemic Calculator (http://gabgoh.github.io/COVID/index.html) if intervention is done ‘TODAY’-
contact tracing and testing, isolation, travel restrictions, and
atleast short term lockdowns. The CFR has been changed from 4% to 2%,
since health system capacity is not exceeded in this scenario. The pink
bars are the number of active infections at any given time (and not the
cumulative cases upto that time) , and the blue bars are the cumulative
deaths.
This is what we see if we intervene today (assuming a strong suppression
intervention). Kindly notice the y axis scale has changed from millions
in the previous graph to thousands in this one. A total of 13,000 cases and 300 deaths. We talked about how epidemics grow exponentially. Now we know how they die exponentially too.
As of writing this article, the confirmed cases in India stood at 344 with 7 deaths. You must understand the difference between true cases and confirmed/official cases. Say
a person gets exposed on Day 1. He develops symptoms on Day 6 (mean
incubation period is 5 days). He seeks care on Day 8 (this can be
reduced with public awareness about symptoms). His results come back
positive on Day 10. So the number of confirmed cases you see in the news
on Day 10, those many cases actually existed 5 days ago when the person
developed symptoms. This is complicated further by the uncertainty
whether Covid patients can be infectious even before they are
symptomatic. Let us stick to the simplified model for now. We
may conclude that confirmed cases lag the true cases by about a week.
The numbers we are seeing today are actually atleast a week old.
How do we know the true cases as of today? There is no certain way to
know, though there are some models that can estimate the same. Based upon those,
let us assume that the actual number of cases today is about 10 times
the confirmed cases. So that is about 350x10=3500 true cases as of today
in India, which is the day I chose as the intervention day(=today) in
the above graph.
In addition to this, the magnitude of difference between true and confirmed cases depends on the rate of testing.
India has not tested aggressively for coronavirus till now (Fig 3), and
that means that the true cases may well be greater than estimated
above, something to the tune of about 10x to 30x the confirmed cases.
This is also suggested by new cases showing up with no contact or travel history, indicating that community transmission is already underway.

Fig 3- Tests performed per million population. India stands at an
abysmal 10.5 tests/million, compared to South Korea’s aggressive testing
at 6148 tests/million. Click here for latest stats on this.

Graph 3- Predicting the coronavirus outbreak in India using Epidemic Calculator (http://gabgoh.github.io/COVID/index.html) if intervention is done ’10 DAYS LATER’.
This is the scenario if we intervene after 10 days. We see about 50,000 cases and 1000 deaths during the
entire outbreak, about a 3–4 fold increase for a 10 day delay in
intervention. Realistically, India will be somewhere between these two
scenarios (Graph 2 and 3), so we can expect about 13,000–50,000 total
cases, and 300–1000 deaths.
By now, every one of us will agree on atleast one thing. We need to intervene, sooner rather than later.
The Indian scenario: reds and greens the Reds-
Demography:
A large percentage of India’s population lives in states with
population density as high as 800 people per square kilometer- a fertile
soil which will exponentially increase the speed of spread. The social
distancing measures we all talk about may be possible for us to
implement, but for homes in which 5 people have to sleep in one room,
that is not feasible.
Healthcare
system capacity: Majority of deaths due to coronavirus have been
attributed not to the inherent severity of the disease, but to the
sudden increase in number of patients requiring hospitalization, many
folds higher than the number of hospital beds available. India has
7,00,000 hospital beds and 70,000 ICU beds. Hospital beds per 1000
people is 0.7 in India, 2.9 in USA, 3.4 in Italy (World Bank).
Considering Italy has already been overwhelmed and US is on its way to
the same, it is hard to imagine the degree to which India’s hospitals
will be crushed if this crisis grows to epidemic proportions.
Healthcare
system accessibility: There is another problem with healthcare in
India, the huge rural-urban divide (Figure 1). Since this is an imported
virus, most urban cities where travellers arrived were affected first,
and then went on to spread centrifugally, ie, the pattern of spread is
urban to rural. If we can arrest this spread by timely intervention,
this factor would play a smaller role.

Fig 1: Rural-Urban divide in healthcare accessibility in India
the Greens-
Demography,
again: The proportion of people above 65 years old to the total
population is 6% in India, 16% in USA, and 22% in Italy. India is a
young country, about half of India’s population is below 21. China saw
80,000 cases with 3,200 deaths, whereas Italy has seen 60,000 cases and
5,400 deaths- almost double the fatality rate. Since most of the
mortality of coronavirus is in elderly or older people with pre-existing
diseases, this factor is encouraging for India.
India
is a late bloomer for coronavirus: We have already seen lots of
countries trying to tackle this crisis, each in their own way. Some of
them were able to contain it (China except Hubei, South Korea), while
others faced disasters of epic proportions (Italy, Germany, US). It is
only now, that India’s time has come, and we have the opportunity to act
pro-actively rather than re-actively.
How do we intervene?
This
is a whole topic in itself, including travel restrictions, social
distancing, lockdown, and extensive contact tracing and testing. I will
talk about the peculiarities of interventions with regard to India.
Lockdown
Starting
with the “janata curfew” or “people’s curfew” on Sunday, about 80
districts across India have now been locked down except essential
services. All international travel has been halted and Indian railways
which carries over 23 million passengers daily is now shut. All inter
state travel has also been shut down. It is widely expected that almost
all of India will go in lockdown in the coming few days- the biggest quarantine ever in human history.
This may seem draconian to some, but it is essential. Such measures
widely break the chain of transmission and isolate existing chains. They
also lead to cluster containment- ie, with no interstate movement, each
state will behave as an independent cluster in epidemiological terms.
This prevents seeding of disease into untouched/less affected states and
more effective contact tracing in affected states. This approach can
only be successful if each state takes responsibility for it’s own
people. It is time for all of us to come at peace with the fact — we
will all be under quarantine very soon, for the greater good.
This move comes in a very timely manner in India. Let me show you why. Look at this table carefully-

Fig 2: Lockdowns due to COVID19 across the world
Wuhan,
the origin of COVID19, is the capital of the Chinese province of Hubei.
Daily new cases started decreasing about 2 weeks after the lockdown.
Hubei is already in the phase of slowly lifting most of the
restrictions. The lockdown lasted for 2 months, they got it under
control. What remains to be seen is how they progress from here, as
history shows that lifting restrictions may lead to a second wave of
disease.
As
for Italy, the situation is very grim with daily cases and deaths still
on the rise. Italy currently has about 800 daily deaths, more than were
ever reported in China. My wishes are with the Italians, but they have
shown us exactly what not to do. I would expect the daily new cases to
start decreasing in Italy within the next few days- I have discussed
this later.
US is not very far behind. Infact with 6000 new cases in a day, US overtook Italy in the maximum number of new cases in a day.
The TIMING of quarantine and lockdown measures is of paramount importance!
India has partially locked down as of now with 350 confirmed cases.
India must ensure this is implemented widely across the country as soon
as possible. And this must be continued for now, I hope you see why.
Only lockdown is not enough!
Say
you have a confirmed case- Mr X. First you quarantine Mr X. You then
trace all the people Mr X has been in contact with since onset of
infectious period, reach out to them and place them under quarantine. In
a slightly more aggressive strategy, you go ahead and test these
contacts even if they don’t show symptoms (India is doing this now). By
doing so and following up until all people in this chain either recover
or are asymptomatic for 14 days, you end this particular chain of
transmission originating from Mr X. Now you got to do this for all the
existing chains! It is a huge task, but not an impossible one. We can learn from Kerala with their extraordinary track record in contact tracing.
Dr
Mike Ryan from WHO said: “The danger right now with the lockdowns … if
we don’t put in place the strong public health measures now, when those
movement restrictions and lockdowns are lifted, the danger is the
disease will jump back up. What we really need to focus on is finding
those who are sick, those who have the virus, and isolate them, find
their contacts and isolate them.” Lockdown will
prevent new chains of transmission from forming, but the virus still
proliferates in existing chains. These existing chains need to be
identified. How? By extensive contact tracing, testing and isolation. It is only a combination of these two that will result in an effective suppression response.
As
the outbreak progresses, more and more chains of transmission are
formed with each branching point. The earlier you do the lockdown, the
fewer chains you need to track down and isolate. Here we have
another reason for why early intervention is beneficial. Timely
lockdowns are more effective, and they last for shorter periods of time.
The earlier we enforce it, we earlier we can start lifting it, the earlier the people and economy can start to recuperate.
If
you are careless and let the outbreak reach Phase IV- widespread
community transmission, you can no longer discern where the cases
originate from. It becomes a huge interconnected web and you can no
longer effectively do contact tracing. This is where New York is right
now- they have asked people not to get tested because they don’t have
enough equipment for doing those huge number of tests. Testing in New
York is now reserved for healthcare professionals, hospitalised
patients, and high risk symptomatic people. Alas, but at this point you
can only sit tight and brace for impact.
When do we see the effect of these interventions?
Let
us assume we enforce lockdown on Day 1. This has an immediate effect of
cutting down exposure of infected people to healthy people. Since the
mean incubation period is 5 days (range 4–14 days), daily new
symptomatic patients will start decreasing from Day 6 (new patients who
are symptomatic from Day 1 to Day 5 have actually been infected before
the lockdown). The patient soon seeks care and is diagnosed as a
confirmed case. All these steps take time and so the effect is not
immediately visible. It has been seen in the case of China, that it takes about 10–14 days after lockdown enforcement for the effect to show.
We
should expect a drastic increase in new cases and fatalities in India
for the next couple of weeks (atleast for 10 days), thanks to expected
exponential phase and expanded testing criteria.
It is important not to be discouraged by this finding. With India
already at the brim of ICU bed occupancy, many of our hospitals will be
overburdened. Due to the chronic under-funding of healthcare in India,
we need to ensure some stop-gap measures immediately. The government
needs to make sure we acquire enough PPE (personal protective
equipment), add extra bed capacity by repurposing beds and creating new
facilities, and acquire ventilators- fast!
As Tomas Pueyo writes in his enlightening analysis,
time is the most valuable thing we stand to gain from a lockdown. The
time to learn more about what we are facing, the time to do research on
medicines and vaccines, the time to prepare our infrastructure for any
impending attack. It’s like holding the enemy at
bay, while we prepare our defenses and send our spies to know thy
secrets. The enemy also starts to die down by itself in the meantime due
to dwindling supplies.
Looking for the right numbers to see this effect:
An exponential growth curve which eventually flattens out is called a
logistic curve (Fig 4 left). The slope of this graph at any given time
shows the rate of increase of cases over time ~ number of daily new
cases. The inflection point is the point at which the slope first starts
decreasing/flattening out. How do we know we have reached the inflection? By keeping an eye on the daily new cases. When you see new cases for a day are less than the new cases on the previous day, you know you’re there. The
absolute number of cases will still increase after this, but the rate
of increase slows down, and that is the first indication that we are
starting to get a hold of the outbreak.
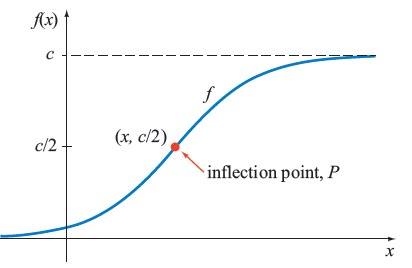

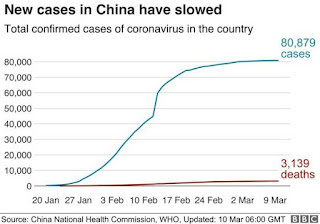
Fig 4(top)- A standard logistic growth curve, showing the inflection point. Fig 4(bottom)-
Cumulative COVID19 cases over time in China. China showed its
inflection point on Feb 5 (13 days after lockdown). The notch in the
middle of the graph is a statistical artifact as a result of change in
case criteria.


Fig 5(top)- Cumulative COVID19 cases
over time. China has completed the logistic curve, while Italy and USA
are still in the pre-inflection exponential growth phase. Fig 5(bottom)-
Zoomed in picture from the lower right corner of the first graph,
showing India just starting out in the logistic curve. Compare India’s
current graph with when the other three countries were just starting
out.
You can see a peculiar similarity between the two graphs (Fig 4left and
right), one hypothetical and the other real. It’s almost stunning how
maths can approximate reality to such a degree of accuracy. China showed
its inflection point on Feb 5, which was 13 days after lockdown (Fig 4
right), and is now on the terminal flat part of the curve. US and Italy
entered exponential growth earlier (Fig 5 left), and are now in the
relatively linear part of the growth curve. I expect Italy to hit
inflection soon (how to predict this here). India has just started on the exponential growth phase (Fig 5 right), and will take quite some time to reach inflection.
Conclusion: What India needs to do right now
~Social distancing.
~Enforce wide and definitive lockdown measures for atleast 2–4 weeks.
~Expect and prepare for drastic increase in cases for the next 2 weeks. Acquire additional health system capacity for the same.
~Effective isolation of patients, contact tracing and quarantine measures. Ramp up testing.
~Elderly (above 65 years) to be protected more vigorously. Save the old from the young.
~Fast-track indigenous vaccine development so that we can prevent a second wave later.
~Provide social security to people who are affected most during the lockdown- mostly daily wage workers.
We
should not expect the government to do all of this. It is our
collective civic duty to adhere to public health guidelines and help out
in whatever way we can. It may be difficult for us in India, who are
unknown to the concept of mass lockdown, to comprehend what is
happening. But we need to know why this is happening and accept the fact
that it is. The policy-makers (government) and the policy-takers (public) need to step up to this challenge together. India can do this!
We can either make this an opportunity to transform our healthcare and outbreak response strategy into a robust one, or let it break through the very backbone of our nation.
A
staggering number of people still don’t understand what we are going
through. If you think other people need to know more about this, go
ahead and share this with your friends. With most of us on lockdown,
they would appreciate something to kill(?) their time. If you would like
to add something to what I’ve written, or disagree with some part of
it, feel free to leave a response below and I will be happy to respond.
I’ll leave you with this-

You can contact me at xmohakgupta@gmail.com for queries/discussions/collabs.
Additional reading:
Coronavirus: The Hammer and the Dance — by Tomas Pueyo (excellent read)
The proximal origin of SARS-CoV-2 — genomic analysis to determine origins of this novel virus. Also answers whether it was genetically engineered or not.
Exponential growth and epidemics — by 3blue1brown
Predicting impact of public health measures on COVID mortality and healthcare demand — by Imperial College London
Coronavirus India case tracker — by CovidOut
References:
Only
references for the epidemiological and clinical parameters used in
predictive modeling are listed here. Other references are provided with
the respective data in the main text.
- https://annals.org/aim/fullarticle/2762808/incubation-period-coronavirus-disease-2019-covid-19-from-publicly-reported
- https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf
- https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-NPI-modelling-16-03-2020.pdf
- https://www.thelancet.com/action/showPdf?pii=S0140-6736%2820%2930566-3
- https://wwwnc.cdc.gov/eid/article/26/6/20-0320_article
Comments
Post a Comment